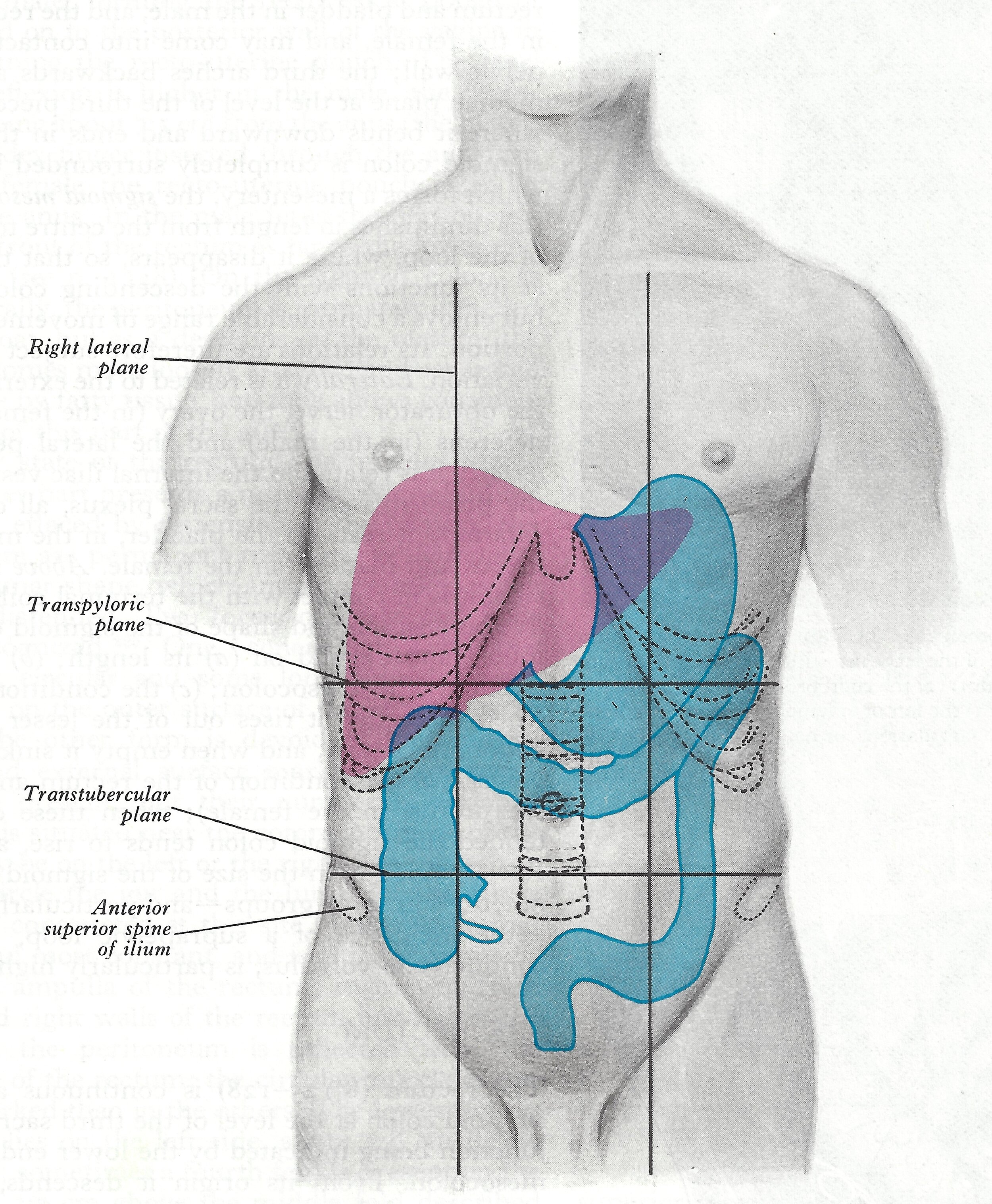
A laparotomy is an opening made through the abdominal wall into the peritoneal cavity
Surgical intervention may be necessary to repair or remove traumatised tissue, to cure disease processes by organ removal, or to examine by biopsy. Otherwise a laparotomy might be used to visualise internal organs for diagnosis. Surgery may be indicated for diagnostic, therapeutic, palliative or prophylactic reasons. Most procedures requiring a laparotomy involve the organs of the alimentary canal.

In the original exhibition, we displayed a ‘Trolley lay-out’ of the instrumentation for a laparotomy placed in the order it would be required. These instruments date to the mid- to late-20th Century, and many are still used today. We have replicated the display here with a point-by-point description of the operation, with images of the required instrumentation where available.



1. Preparation of the site, by cleansing the area with an antiseptic solution.
Sponge holder with swab GM2004.128 Marshall Collection
Kidney dish receiver GM2011.1.26 Richards Collection
Plastic bottle for betadine solution
Gallipot for solution 1 of RM1267 Marshall Collection
2. Cover the surrounding site with sterile towels thus defining the area to be operated on.
3. secure the towels with a clip.
Towel clip GM2005.8 Marshall Collection
4. Apply clear adhesive strip to the operative site, through which the incision is made.
5. connect and secure the tested yankauer/poole suction tube and tubing to the operative field to remove excess fluid.
6. connect and secure the tested diathermy forceps/needle and lead to the operative field.
Used as an electro-coagulation (to control bleeding vessels).
7. the skin incision is made through to the fascia.
Bard Parker handle GM2004.10.3 Marshall Collection
8. Haemostats (artery forceps) used to control the bleeding. Clamped vessels are ligated (tied) with fine absorbable ligatures (cat gut or silk) or are electro-coagulated.
Artery Forceps MBI0385 Marshall Collection
Plain dissecting forceps GM2004.11.1 Marshall Collection
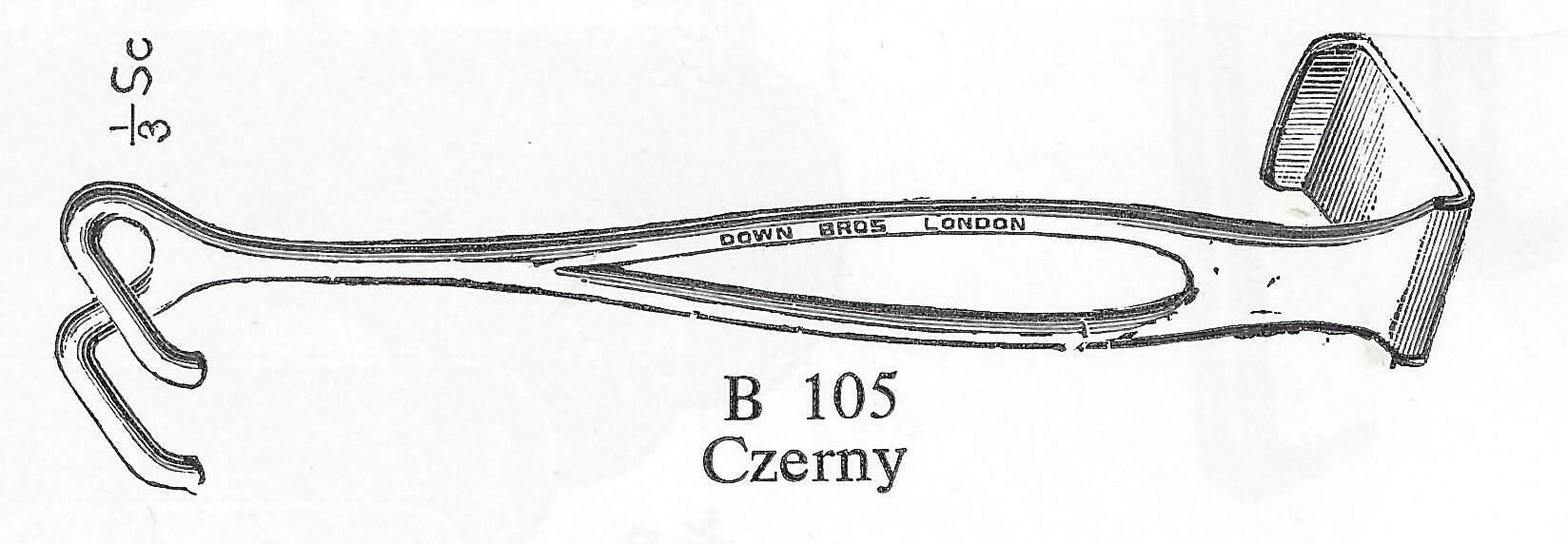
9. The wound edges are retracted with small retractors.
10. with tissue forceps and scalpel, the external fascia is incised.
11. Using long dissecting scissors, the external oblique muscle is split the length of the incision. Bleeding vessels are controlled by haemostates/ligation clips and/or tied with fine ligatures.
Curved dissecting forceps GM2011.1.21 Richards Collection
McIndoe’s curves dissecting scissors GM2009.79.8 Forest Glade Medical Centre, Kidderminster
Plain dissecting forceps GM2004.11.3 Marshall Collection
Black mercilene thread Handling Collection
12. The external oblique muscle is retracted.
13. The internal oblique and transverse muscles are split, parallel to the fibres, up to the rectus sheath with a scalpel or scissors.
These muscles are then also retracted
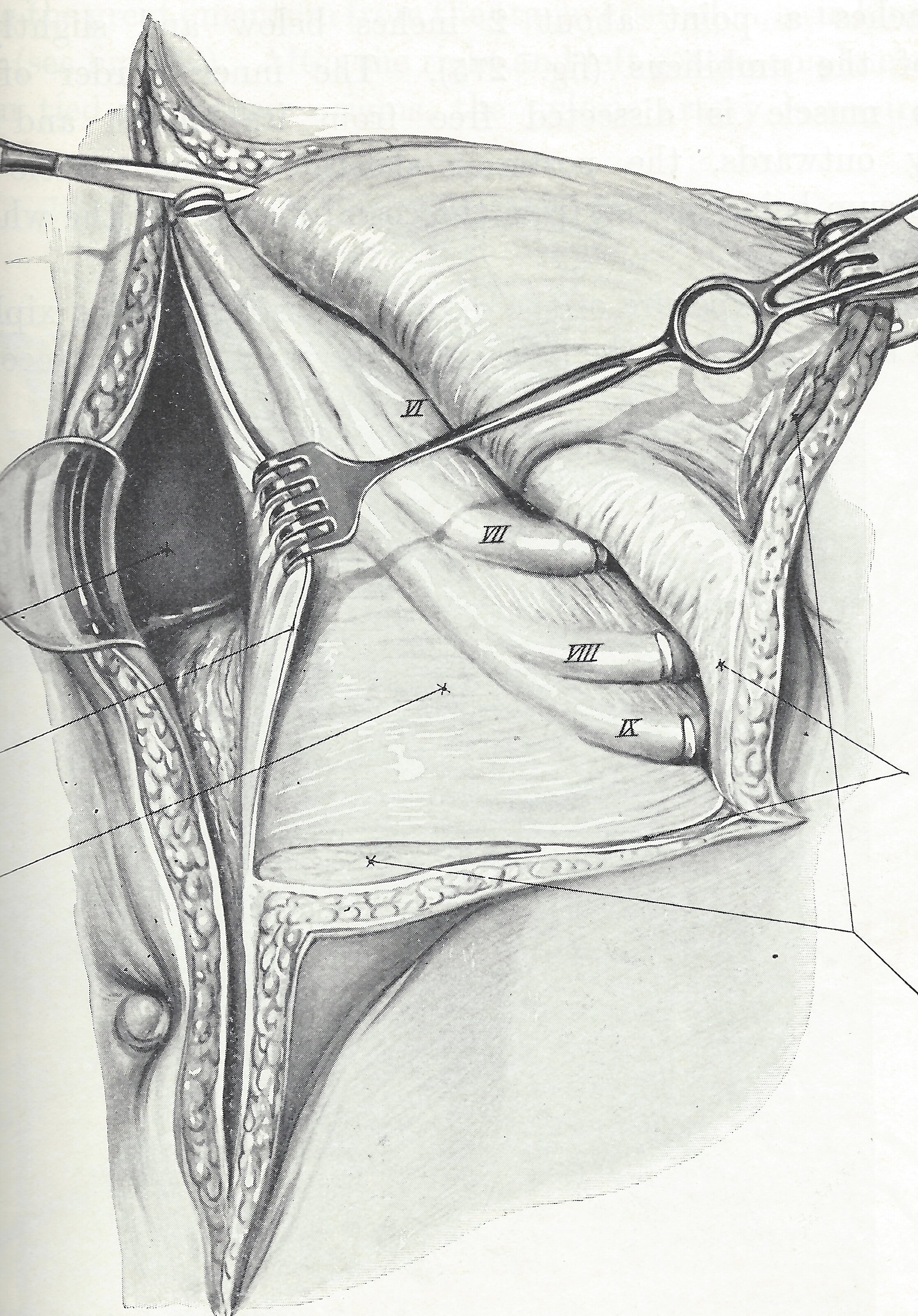
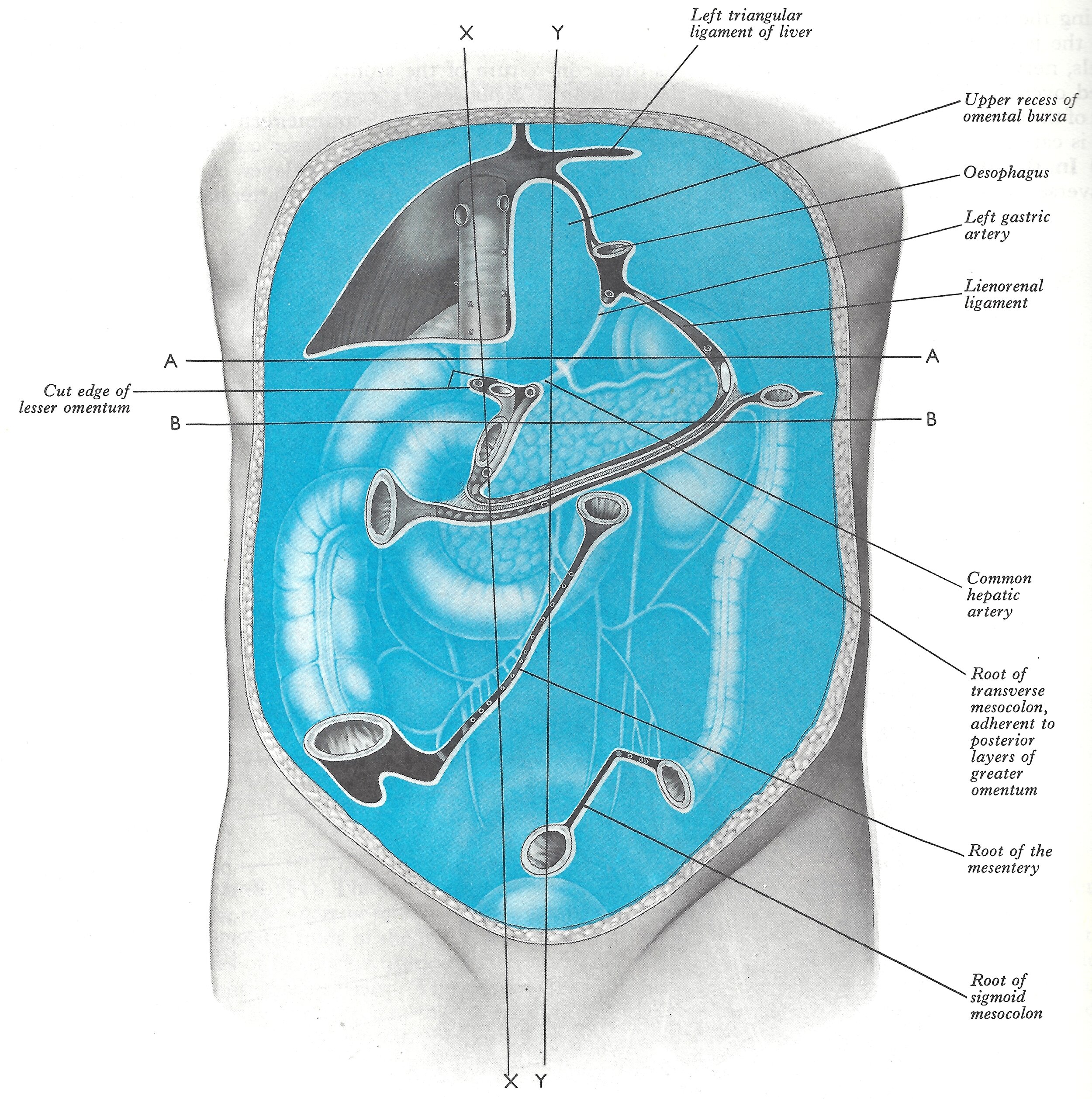
14. the peritoneum is exposed, grasped with smooth-ended (non-toothed) tissue forceps and nicked with the scalpel blade.
15. the peritoneal incision is extended the length of the wound using scissors and retracted with larger retractors.
Retractor GM2004.157 Marshall Collection
Self-retaining retractor GM2004.159 Marshall Collection
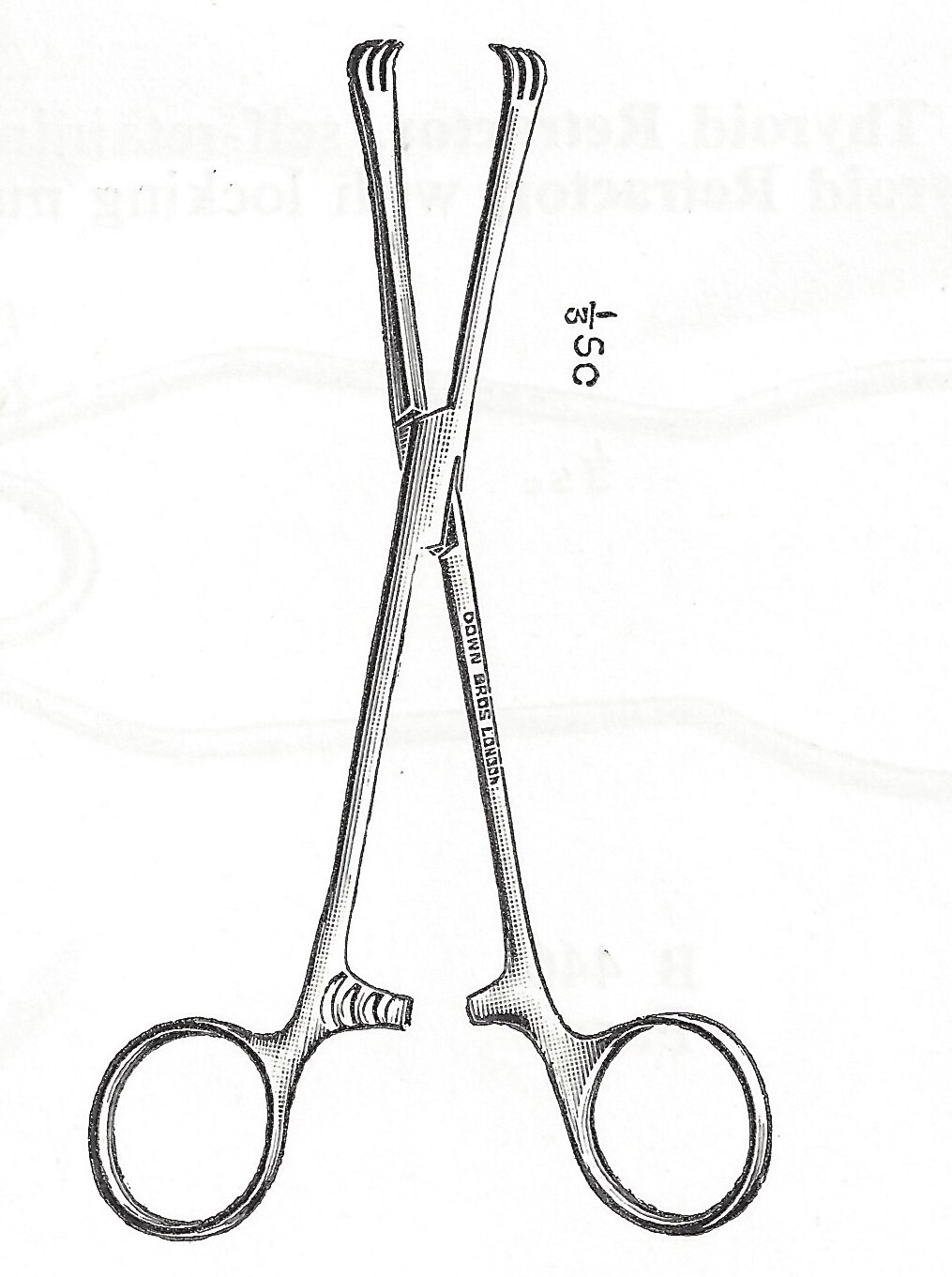
16. Sponges (small swabs) held on sponge holding forceps, large abdominal taped swabs (secured on the tape by a small artery forcep) are used as needed. Cultures may be taken at this time.
17. Once the affected organs are identified, a large self-retaining retractor is used to ensure adequate exposure.
Traumatic Payrs crushing clamp GM2006.3 Marshall Collection
Non-crushing intestinal clamp/bowel clamp GM2004.19 Marshall Collection
Ligature guide MBI0982 Marshall Collection
18. Following internal procedure on affected organs the abdomen is then closed.
19. two tissue forceps are used to approximate the peritoneal edges and the peritoneum is closed with an absorbable suture (either as a continuous length or as several separate interrupted stitches).
The internal oblique muscle is closed in the same way.
Needle holder GM2005.13 Marshall Collection
Chromic cat gut RM1679 Marshall Collection
Chromic cat gut (once broken from glass) RM1729 Marshall Collection
20. Muscle tissue is approximated in the same way and may or may not be sutured depending on muscle strength and muscle retraction.
21. The external oblique fascia is closed with interrupted sutures/staples or both. Retraction is necessary as the various layers are closed.
22. Fine interrupted absorbable sutures are usually employed to close the subcutaneous layer. Retraction may be provided by swabs or retractors.
Absorbable cat gut for subcutaneous tissue RM1679 Marshall Collection
Cat gut for subcutaneous tissue RM1734 Marshall Collection
23. Skin edges held with skin hooks/toothed forceps and approximated using sutures of either silk/nylon or other non-absorbable material. These sutures are used on a curved or straight cutting-edge needle. Alternative is the use of interrupted skin clips.
Gallipot RM1267 Marshall Collection
Receiver GM2011.1.26 Richards Collection
Michel Applicator with clip and guide (two items) GM2006.25.1 Marshall Collection
Tissue forceps GM2004.17.1 Marshall Collection
Gillies scissors MBI0912 Marshall Collection
Pack cutting needles MBI0823 Marshall Collection
Pack nylon skin suture RM1731 Marshall Collection
Curved cutting hand needle MBI0800 Marshall Collection
Melolin Handling Collection
Post-operatively it may be necessary to monitor fluid loss from the operative site. This is achieved by inserting different types of drainage tubes or catheters (sutured in place) which are attached externally to a collection bag or bottle.

MARGARET INGMAN NEE BATY AFTER QUALIFYING
Margaret Ingman researched and created this display for the George Marshall Medical Museum. She has been a volunteer at the Museum since it opened in 2002.
She is a retired State Registered Nurse with diplomas in Ophthalmology and Theatre with Anaesthetics. Using her knowledge as an Ophthalmic Nurse, she qualified in Eye Retrieval surgery, enabling her to carry out this procedure for research and for the benefit of patients requiring corneal transplants.
Her experience has involved travel and work in South Africa, Lesotho, Swaziland, Zimbabwe, and Canada using her specialist knowledge. In the UK she has worked theatres in the private sector and in the National Health Service as a commissioning officer of ten operating theatres in a newly-built hospital.